Appendix A
Survivorship Care Plan Provider Summary
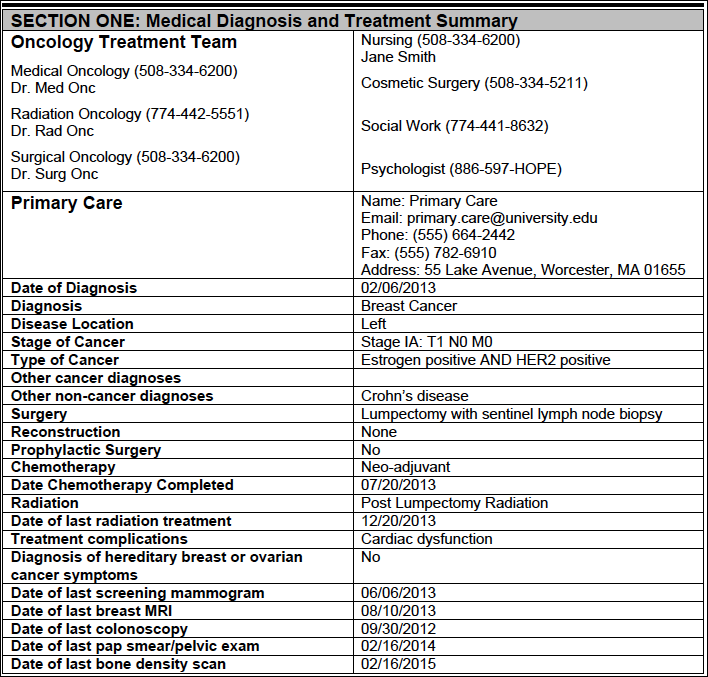
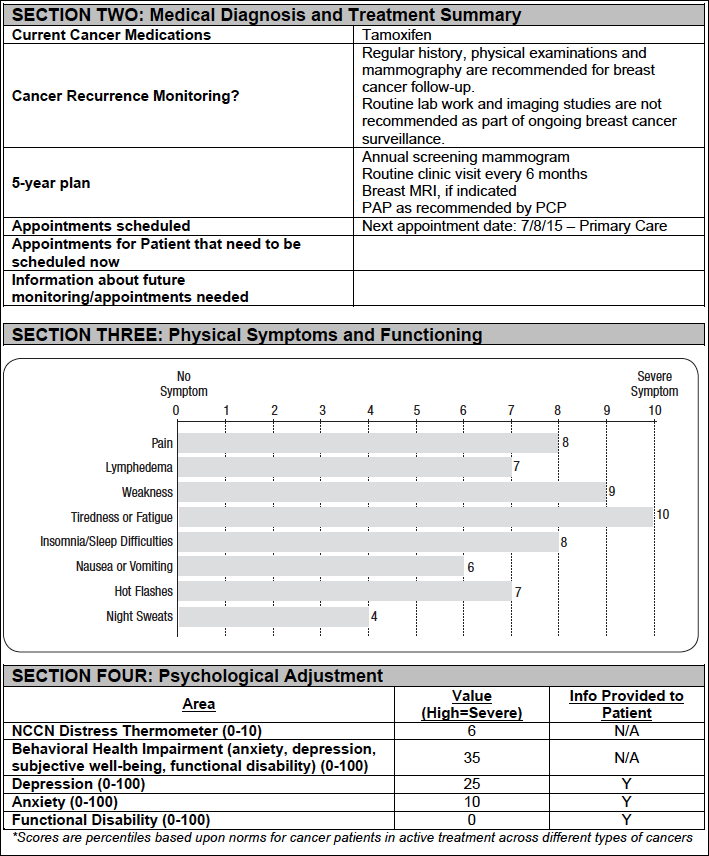
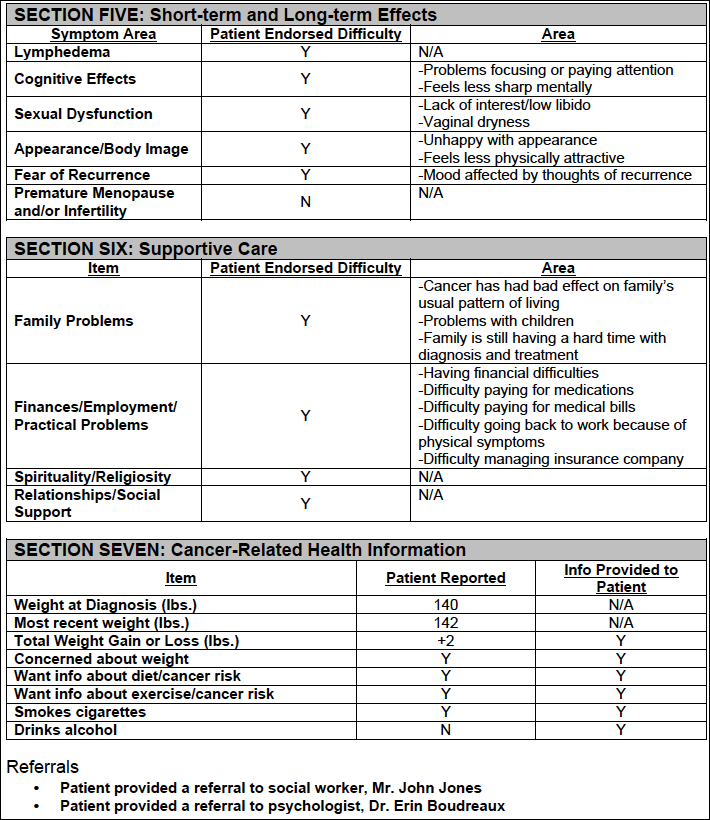
Name: PATIENT, MOCK DOB: 01/01/1950 Date of Plan: 10/16/2014 SCP Created by: Oncologist, MD
Survivorship Care Plan: Provider Version of SCP
The first part of this Survivorship Cancer Plan (SCP) labeled PROVIDER VERSION is for your medical providers including members of your oncology team and your primary care doctor. The PROVIDER VERSION provides information about your medical diagnoses, treatment and future medical plans. Your oncologist will review this section with you at this visit. The PATIENT VERSION of the SCP has some detailed information about breast cancer survivorship for you to review on your own.